Arteriovenous fistula for dialysis
The recommended solution for stable, safe and durable vascular access
Medical Procedures
Vascular Techniques
Endovascular Techniques
Conditions Treated
Fistula arteriovenoasă pentru dializă este soluția recomandată pentru un acces vascular stabil, sigur și durabil la pacienții care fac hemodializă pe termen lung.
La Clinica VenArt din Cluj-Napoca și București, crearea fistulei arterio venoase este realizată de chirurgi vasculari cu experiență internațională, în
Arteriovenous fistula for dialysis is the recommended solution for stable, safe and durable vascular access in patients undergoing long-term hemodialysis.
At the VenArt Clinic in Cluj-Napoca and Bucharest, the creation of arteriovenous fistula is performed by vascular surgeons with international experience, in maximum safety conditions. Each case is evaluated individually to choose the right option for the anatomy of the vessels and the real needs of the patient.
Book a vascular surgery consultation to determine the best vascular access for dialysis. Phone: 0731 837 520.
Book an Appointment
What is an arteriovenous fistula and when is it necessary?
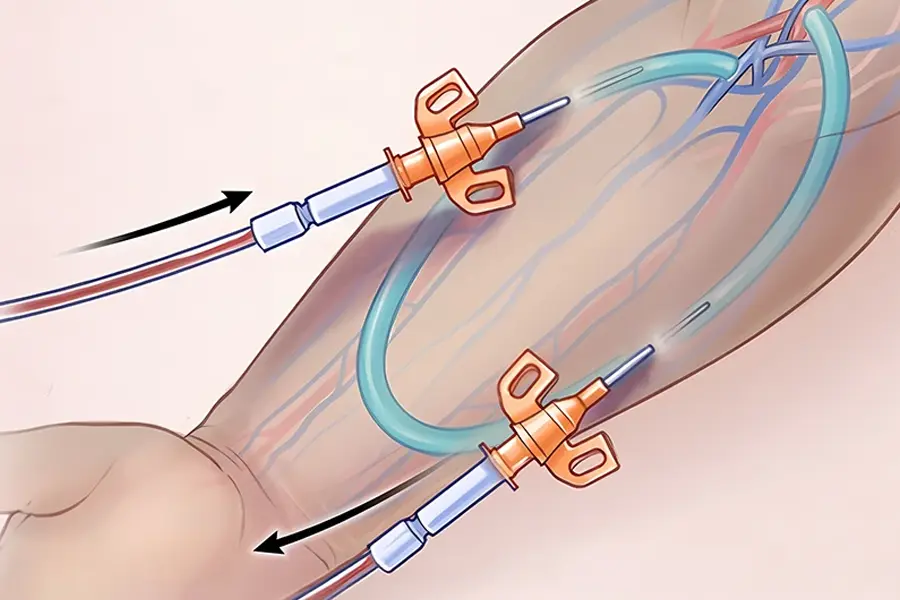
An arteriovenous fistula (AVF) for dialysis is a surgically created connection between an artery and a vein, usually in the arm. This connection allows sufficient blood flow for repeated hemodialysis sessions.
After the procedure, the vein begins to dilate and become more resistant. This process is called maturation and is necessary for the fistula to be used safely.
An arteriovenous fistula for dialysis is especially recommended for patients with advanced chronic kidney disease who need long-term hemodialysis. Ideally, the procedure is performed 6 to 8 weeks before dialysis begins.
Who needs this intervention?
- Patients with advanced chronic renal failure;
- Patients who are due to start hemodialysis in the coming weeks or months;
- Patients using a temporary catheter and need permanent vascular access;
- Patients seeking a safer and more durable solution than a central venous catheter.
You can learn more about the medical specialty involved in such interventions on the vascular and endovascular surgery page.
Why is a hemodialysis fistula recommended?
The arteriovenous fistula for dialysis is considered the gold standard for permanent vascular access. It provides good blood flow, lasts for years, and has a lower risk of infection than other options.
For many patients, choosing a fistula over a catheter means greater safety and fewer long-term complications. In addition, after maturation, comfort is better in everyday life.
Arteriovenous fistula versus central venous catheter
Duration of use
Arteriovenous fistula:
Years
Central venous catheter:
Usually temporary
Risk of infection
Arteriovenous fistula:
Lower
Central venous catheter:
Higher
Dialysis quality
Arteriovenous fistula:
Better blood flow
Central venous catheter:
More limited flow
Long-term comfort
Arteriovenous fistula:
Better after maturation
Central venous catheter:
Can cause daily discomfort
Main role
Arteriovenous fistula:
Permanent access for hemodialysis
Central venous catheter:
Emergency or transitional solution
If the patient needs quick access to treatment, the doctor may initially recommend a catheter. However, for chronic dialysis, a fistula remains the preferred option.
Types of arteriovenous fistula
The type of fistula is chosen after evaluating the vessels in the upper limb. The decision depends on the diameter of the veins, the quality of the arteries, and the patient’s medical history.
Radiocephalic fistula (at the forearm level)
First preferred option. Connects the radial artery to the cephalic vein at the wrist. Maturation time: 6 to 8 weeks. Long-term success rate is the highest of all types.
Brachiocephalic fistula (at the elbow)
Indicated when the veins in the forearm are not adequate. Connects the brachial artery to the cephalic vein at the elbow. Faster maturation. Higher blood flow, useful in difficult dialysis.
Brachiobasilial fistula (with transposition)
Option for complex cases, when other veins are compromised. Sometimes requires two surgical stages. Performed by teams experienced in advanced vascular surgery.
Causes and factors influencing the choice of fistula
Not every patient will have the same type of fistula. The quality of vascular access depends on the individual anatomy and the general condition of the circulatory system.
The doctor takes into account several important factors before the intervention. The goal is to choose a fistula that is functional, durable and as safe as possible.
Factors analyzed before surgery
- The diameter and course of the veins in the arm;
- The caliber and patency of the arteries;
- Previous interventions or catheters used in the past;
- Associated conditions, such as diabetes or vascular disease;
- The patient’s dominant hand and daily activities;
Symptoms and situations in which the patient arrives for evaluation
Often, the patient does not reach the vascular surgeon because of local symptoms in the arm. It is enough that the nephrologist recommends in advance the creation of a permanent vascular access for dialysis.
However, there are also situations in which an already created fistula needs to be checked, because it is not functioning well or signs of complications appear. These signs must be evaluated quickly.
Common signs that require checking
- The fistula no longer vibrates when palpated;
- The arm suddenly swells;
- Local redness or warmth appears;
- There is severe pain in the operated area;
- Difficulty using the fistula during dialysis occurs.
Preoperative diagnosis and evaluation
A complete vascular evaluation is required prior to surgery. This helps to select the type of fistula and reduce the risk of failure to mature.
The main investigation is Doppler ultrasound, used to map the veins and arteries of the arm. In some cases, blood tests and cardiological evaluation are required.
You can read more about the role of vascular ultrasound on the Lower Limb Doppler Ultrasound page.
How the intervention is performed at the VenArt Clinic
Creating an arteriovenous fistula is a short surgical procedure. It is performed on an outpatient basis or with a one-day hospitalization.
Stages of fistula creation surgery
- Preoperative evaluation: Doppler ultrasound to map the veins and arteries of the arm, blood tests, cardiological consultation if necessary.
- Local or locoregional anesthesia: the patient is conscious throughout the intervention, without pain.
- Small incision: at the forearm or elbow, depending on the type of fistula chosen.
- Connecting the artery to the vein: the vascular suture is performed by the vascular surgeon under optical magnification.
- Flow check: immediately after suturing, the surgeon checks the “thrill”, i.e. the characteristic vibration of the functional fistula.
- Dressing and monitoring: the patient is monitored for a few hours, then he can go home.
Duration of the procedure: 45 to 90 minutes.
Maturation: 4 to 8 weeks before first use in dialysis.
Why minimally invasive treatment matters
When possible, a minimally invasive approach offers significant advantages for the patient. Pain is reduced, mobilization is faster, and reintegration into normal activities is easier.
In addition, monitoring and correction of subsequent problems can sometimes also be done minimally invasively. One example is fistuloplasty, used to reopen a narrowed fistula.
Comparison with extended classical surgery
Local discomfort
Minimally invasive approach:
Less
Extended classical approach:
Usually larger
Time to discharge
Minimally invasive approach:
Shorter
Extended Classical Approach:
May be longer
Resumption of light activities
Minimally invasive approach:
Faster
Extended Classical Approach:
May require more time
The need for a large incision
Minimally invasive approach:
Usually not
Extended classical approach:
May be necessary
Arteriovenous fistula angioplasty (fistuloplasty)
Sometimes a fistula that has been working well begins to narrow. This problem is called stenosis and can reduce the flow needed for hemodialysis.
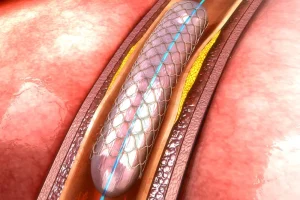
In many cases, the solution is not to completely re-establish the vascular access, but to repair it with balloon angioplasty. The procedure is also called fistuloplasty or percutaneous transluminal angioplasty.
How fistuloplasty works
The surgeon punctures the fistula and inserts a thin guidewire, then advances a balloon catheter to the narrowed area. The balloon is inflated in a controlled manner to reopen the vessel and improve blood flow.
In some cases, special balloons may be used to reduce the risk of re-narrowing. The fistula can sometimes be used the same day after the procedure.
Patients who want to better understand non-surgical (minimally invasive) endovascular treatments can consult the Angioplasty page.
Recovery and care after surgery
Recovery after arteriovenous fistula creation is simple if the patient follows a few essential rules.
What to do in the first few weeks
- Check daily for vibration (thrill) at the level of the fistula. Absence of vibration requires immediate medical contact;
- Do not allow blood pressure measurements or blood sampling on the arm with the fistula;
- Keep the area clean and dry in the first few days after the intervention;
- Avoid tight clothing, watches or jewelry on the operated arm;
- Do not sleep on the arm with the fistula;
- Light exercises with a rubber ball can speed up the maturation of the vein.
Alarm signs that require urgent consultation
- Loss of vibration or pulse at the fistula;
- Sudden swelling, redness, or local warmth;
- Severe pain in the arm;
- Bleeding that does not stop with compression.
Risks and possible complications
Arteriovenous fistula for dialysis is the most durable method of vascular access, but it is not without risks. Sometimes the fistula does not mature sufficiently or loses its functionality over time.
The most common complications are stenosis, thrombosis, and failure to mature. Less commonly, bleeding, local infection, or excessive dilation of the vein may occur.
Many of these problems can be treated if detected early. That’s why post-surgery vascular check-ups and evaluation are essential. Schedule a consultation!
Other treatment and vascular access options
In some situations, a fistula cannot be created immediately or is not the most appropriate solution from the start. In such cases, the doctor may recommend a central venous catheter or another temporary vascular access strategy.
The choice depends on the urgency of starting dialysis, the vascular anatomy, and the patient’s history. The goal is always to obtain the safest access with the best chance of long-term use.
Arteriovenous fistula
When used:
For permanent vascular access
Main limitations:
Requires maturation time
Central venous catheter
When used:
When dialysis needs to be started quickly
Main limitations:
Higher risk of infection and temporary use
Surgical revision or new vascular access
When used:
When the existing fistula cannot be restored
Main limitations:
Depends on available anatomy
Advantages of creating an arteriovenous fistula at the VenArt Clinic
Vascular surgeons with international experience perform consultations, investigations and minimally invasive interventions in Cluj-Napoca and Bucharest. Each case is evaluated individually, and the type of fistula is chosen based on complete vascular mapping of the arm.
- Complete preoperative vascular assessment with Doppler ultrasound;
- Intervention performed by surgeons specialized in vascular access for dialysis;
- Outpatient procedure, without prolonged hospitalization;
- Postoperative monitoring and control consultations included;
- Clear protocol for monitoring fistula maturation;
- Ability to also perform fistuloplasty in the same clinic, if needed later.
Medical Team
Frequently asked questions about arteriovenous fistula
What is an arteriovenous fistula for dialysis and why is it needed?
It is a surgically created connection between an artery and a vein, usually in the arm. It provides the vascular access needed for repeated hemodialysis, under safer and more stable conditions.
How long can the fistula be used after surgery?
The fistula usually takes 4 to 8 weeks to mature. The doctor confirms the timing of use after clinical evaluation and, if necessary, ultrasound.
Is a fistula better than a dialysis catheter?
In most cases, yes. Fistula is better suited for chronic dialysis because it has a lower risk of infection and can function for a much longer period.
Is there a risk that the fistula will not mature properly?
Yes. Sometimes the vein does not develop sufficiently for effective use in dialysis. In these cases, reevaluation, fistuloplasty, or creation of another vascular access may be necessary.
What complications can occur after fistula creation?
The most common complications are stenosis, thrombosis and insufficient maturation. Less commonly, bleeding, local infection or dilation of the vein over time may occur.
Can an existing fistula be repaired?
Yes. In many cases, a narrowed or blocked fistula can be treated with balloon angioplasty without immediately creating a new fistula.
How long does recovery take?
Local recovery is usually rapid, and the patient can go home the same day or after a short monitoring period. However, dialysis is only used after complete maturation.
How much does the intervention cost?
The cost depends on the complexity of the case. Call us and we will determine the next steps together.